Search in dictionary
Acupuncture
针灸 〔針灸〕 zhēn jiǔ
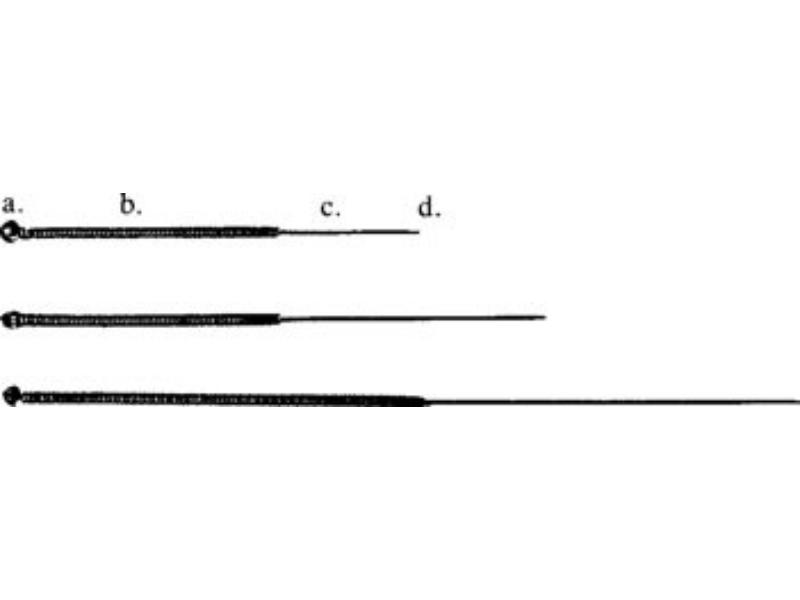 |
| Filiform needles: a. tail; b. handle; c. body; d. point |
1. The practice of puncturing the body with metal needles (steel, gold, or silver) at specific points in order to regulate provisioning, defense, qì, and the blood.
2. Acumoxatherapy, i.e., acupuncture and moxibustion (as well as the related therapies cupping, ear acupuncture, guā-shā, acupressure (shiatsu), and tuī-ná.
Definition (1) applies in what follows.
Contents
- Needles
- Needling
- Precautions, Contraindications, and Mishaps
- Other Materials and Techniques Related to Acupuncture
Needles
| Needle Diameters | Chinese Gauge | Japanese Gauge | Diameter (in mm) |
|---|---|---|
| 26 | 15 | 0.46 |
| 28 | 10 | 0.34 |
| 30 | 8 | 0.30 |
| 32 | 6 | 0.27 |
| 34 | 4 | 0.22 |
| 36 | — | 0.19 |
| — | 3 | 0.20 |
| — | 2 | 0.18 |
| — | 1 | 0.16 |
The filiform needle (毫针 háo zhēn) is the one most commonly used for performing acupuncture. It is generally made from a stainless-steel wire that is sharpened at one end and has a thin wire of copper, stainless steel, or silver wrapped around its opposite end to serve as a handle.
Stainless steel is chosen for the body of the needle because of its flexibility, strength, and resistance to oxidation. Though silver and gold are also oxidation-resistant, they are expensiveand are relatively soft metals. Thus, they are used only according to specific schools of practice when their pliability does not impede treatment.
Filiform needles are available in several lengths and diameters. Frequently seen lengths are 0.5 to 5 cùn, and diameters from 30 to 34 gauge are the most popular. See table below for information about needle diameter and needle length.
Thin needles provide a less potent stimulus than their thicker counterparts. They are therefore favored for the treatment of older persons, children, or weak patients. They are also appropriate for the treatment of the ocular region. Thick needles produce a strong stimulus that is more suitable for robust patients. 30- and 32-gauge needles are the most commonly employed.
Today, pre-sterilized disposable needles are popular because of their convenience and safety. These needles often come with an insertion tube and differ from standard needles in that their handle is usually made from aluminum or steel tubing that is crimped in place. This type of handle also typifies Japanese needles.
The thinnest Chinese needles (those with a diameter smaller than 34 gauge), and most Japanese needles, are often inserted with the aid of a tube, which supports the body of the needle during insertion and prevents contact with the practitioner’s skin. Insertion tubes are available in stainless steel or glass (for re-sterilization), and in disposable plastic, in lengths approximately 4 mm shorter than the needle with which it is used.
Before use, needles should be inspected for imperfections. The tip of the needle should not be too sharp, as this can cause it to bend or break off. It also should not be blunt, as that makes the needle difficult to insert and causes pain.
| Needle Length and Application | ||
|---|---|---|
| Length | Area of Use | |
| Cùn | mm | |
| 0.5–1. 0 | 13–25 | Head, face, ear, eyes, fingers, toes |
| 1.5 | 40 | Limbs, body trunk, back |
| 2–5 | 50–125 | Thigh, buttocks, upper arm, and other particularly fleshy areas. Also employed when joiningpoints. |
Pulling the needle by the handle through a dry cotton ball will reveal whether there are burs on the body or tip. Burs can be filed off with fine sandpaper or a grinding stone.
Any cracks or corrosion in the body or tip of the needle necessitate its disposal. If the needle has a crimped handle, it should be tested to ensure that it will not separate from the body of the needle during manipulation.
Sterilization
Needling equipment, hands, and the part of the body to be needled have to be properly sterilized (消毒 xiāo dú).
Needling equipment: Needles, needle trays, and any metal objects that come into contact with needles should be sterilized by steaming (15 mins at 120ºC/275ºF) or boiling (for 15 minutes), or by soaking in 70–75% alcohol for 30 minutes. Disposable needles now commonly used are pre-sterilized.
Hands: Practitioners must wash their hands thoroughly with soap or using alcohol wipes.
Needling site: Wipe the site to be needled with 70–75% alcohol. In ear acupuncture, wiping the outer ear with 2% iodine before wiping with alcohol is recommended.
Needling
Positioning the Patient for Treatment
Before needling, the patient must be appropriately positioned for comfort and safety. The position selected for the patient should be one that allows him to be comfortable enough so that he can remain still for the duration of the treatment. The practitioner must also have access to the necessary points. In general, these two criteria can be met by one of the postures illustrated below, but sometimes the treatment must be divided into two or more sections during which the patient assumes different postures to allow the practitioner access to the points to be needled. Note the use of pillows in various positions that allow maximum patient comfort.
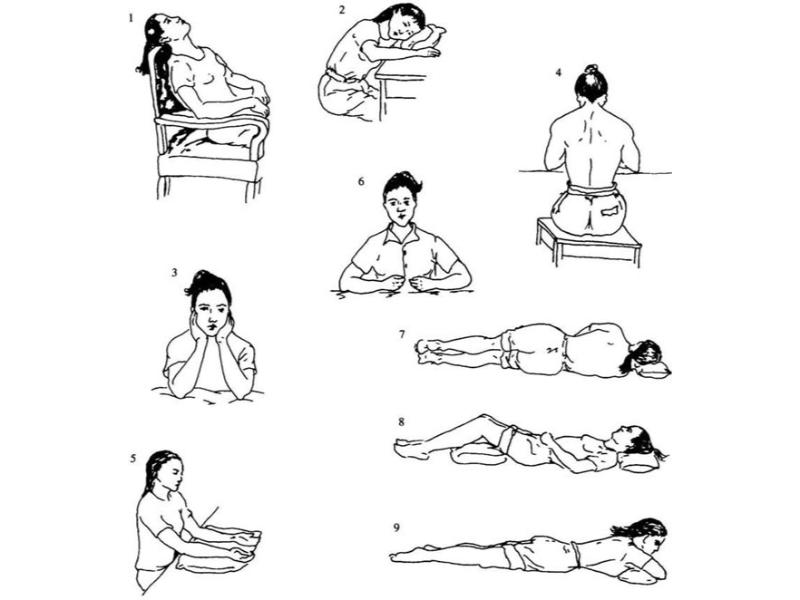 |
| Patient postures |
- Sitting: Head, neck, face, and front and sides of body.
- Sitting at a table, leaning to one side: Side of head or neck.
- Supporting the head: Head and face.
- Sitting at a table with the head bowed: Back and lower back (see also prone position).
- Sitting elbows bent exposing palms: The yīn channels of the forearms, face.
- Sitting elbows bent exposing back of hands: The yáng channels of the forearm. If the hands are adjusted, heart and small intestine points will also be available for treatment.
- Lying on the side: Sides of legs, rib-sides; bend the uppermost leg when selecting points in the area of GB-24 or GB-30 and straighten the upper leg when selecting points in the area of LR-13 or SP-21.
- Supine with legs bent: Face, neck, cheek, abdomen, front and sides of lower limbs.
- Prone: Head, neck, back, lower back, buttocks, back and sides of lower limbs
Needle insertion (進針法 jìn zhēn fǎ)
Needle insertion comprises three distinct phases: insertion of the needle beneath the superficial layers of the skin; movement of the needle to the depth at which contact with the acupuncture point is made; and elicitation of a characteristic physiological sensation, a procedure called obtaining qì
(得气 dé qì), which is described further ahead under needle manipulation techniques. Though these aspects of needle insertion become, in actual practice, a single event, it is helpful to understand them individually, and to develop skills in their individual application.
Traditionally, the practitioner holds the hand of the needle in his strong hand (which for most people is the right hand) between the index finger and thumb, possibly using the middle finger touching the body of the needle for support and guidance. The thumb and in some cases the index finger of the other hand can be placed around the tip of the needle at the insertion site. The needle is then gently pressed into the site with a slight clockwise and anticlockwise twirling to facilitate entry.
Note that since this traditional method involves the practitioner’s fingers coming into contact with the body and tip of the needle, it is not considered hygienic. For this reason, many modern practitioners use the method of tube insertion.
| Needle Insertion Angle | ||
|---|---|---|
| Name | Angle | Comments |
| Perpendicular insertion | 90° | The most common insertion. |
| Oblique insertion | 45° | Appropriate where the subcutaneous flesh is thin or where an internal organ lies beneath the point. Commonly used on the chest and back. Also employed for moving qì in a given direction. |
| Transverse insertion | 10–20° | Suited for areas with little flesh beneath the skin. The head, face and neck often require transverse insertion. Also useful when joining points. |
Four techniques of insertion are commonly practiced: the two-finger press (also called holding the body of the needle,
); the single-finger press(also called the pressing finger
technique); the skin-spreading technique;and the skin-pinching technique.These are described below.
- Step 1: Hold the needle at the handle with the thumb and index finger of the right hand, while the left thumb and forefinger support the end of the needle body with a small piece of sterile cotton.
- Step 2: Place the tip of the needle lightly on the surface of the skin over the point.
- Step 3: Insert the needle by exerting a quick, firm downward pressure with both hands at the same time.
- Step 4: Remove the cotton and continue to insert the needle until the correct depth has been reached.
- Step 1: Press either the thumbnail, or the nail of the index finger of the left hand, onto the skin surface over the point.
- Step 2: Holding the handle of the needle with the right thumb and forefinger, support the needle tip against the fingernail.
- Step 3: Keeping the needle next to the nail, insert it through the skin with a quick, firm downward motion.
| Needle Insertion Depth | ||||
|---|---|---|---|---|
| Relative depth of Insertion | Constitutional Aspect | |||
| Age | Gender | Body Type | Qì and Blood | |
| Shallow | Elderly and infants | Female | Thin | Qì and blood vacuity |
| Deep | Teens to middle age | Male | Corpulent | Abundance of qì and blood |
- Step 1: While holding the handle of the needle between the thumb and forefinger of the right hand, bring the needle tip to rest lightly on the skin surface above the point.
- Step 2: Stretch the skin on either side of the point with the thumb and forefinger of the left hand.
- Step 3: Insert the needle using a quick, firm downward movement with the right hand, while continuing to stretch the skin with the left hand.
- Step 1: While holding the handle of the needle with the thumb and forefinger of the right hand, pinch the skin around the point with the left hand.
- Step 2: Rest the tip of the needle lightly on the point, and insert with a quick, firm, downward movement.
With all rotating insertion techniques, after the superficial layers of skin have been penetrated, the needle is moved to the correct depth with a slow, slight rotation. The needle rotation is performed either in a single direction, or equally in both directions, and is combined with the continuous downward movement of the needle. Insertion rotation is not intended to provide supplementation or drainage stimulation.
Tube insertion (管针进针法 guǎn zhēn jìn zhēn fǎ): Tube insertion employs the use of a thin stainless steel, glass, or plastic tubular guide into which a tailless needle (without the end ring) is placed before insertion. Insertion tubes are approximately 4 mm shorter than the needles for which they are intended, thus exposing a consistent length of the needle handle when the tube and the needle tip are allowed to rest on the skin surface. The needle is gently tapped into the skin until the top of the needle handle is level with, or just below, the top of the tube. The guide tube is then removed and the needle inserted to the appropriate depth. This technique is most often used with long and/or thin needles, as well as in the treatment of children and adults who are particularly sensitive.
Practitioners who favor the use of insertion tubes often develop skills in manipulating the tube and the needle with one hand. Such skill allows acupuncture points to be palpated and located with the index finger of the left hand, while the tube and needle are prepared with the right hand. Care must be taken when practicing this technique that clean fields are not compromised. The practitioner must not come in contact with the body of the needle.
Angle and depth of insertion: The correct angle and depth of insertion is determined in part by the physiology of the area being needled and in part by the intended effect of the treatment.
Angle of insertion: There are three principal angles of insertion as outlined below. These angles are guidelines that are subject to modification according to the requirements of the particular site and the disorders being treated.
Depth of insertion: Depth of insertion is determined by consideration of the local anatomy, the patient’s constitution, the season, and the depth and nature of the evil.
The practitioner must be aware of the anatomy at each point and the dangers of an excessively deep insertion. The needling depths recommended for each point of this text are guidelines that must be fitted to the physique of the patient.
Table 13-10 is a condensation of guidelines set forth in the Nèi Jīng regarding depth of insertion based upon patient constitution.
In modern practice the practitioner must weigh the clinical propriety of determining needle depth by the seasons. Consistent with the theory put forth in the Nèi Jīng, the Nàn Jīng states:
In spring and summer yang qì is in the upper regions and a person’s qì also is in the upper regions, therefore one should needle superficially. In autumn and winter yáng qì is in the lower regions and a person’s qì is also in the lower regions, therefore one should needle deeply.
In general, heat and vacuity diseases require shallow insertion, and cold and repletion diseases require deep insertion. Needling depths for repletion heat and vacuity cold diseases are determined by the depth of the evil.
The depth of the needle insertion should be in accord with the depth of the disease. The Nèi Jīng states:
Deep needling applied to a superficial disease results in injury [to deeper lying flesh]… [and] superficial needling applied to a deep disease does not drain [the evil].
Whereas an external evil giving rise to an exterior pattern can be treated with shallow needle insertion, a deeper invasion of the evil requires deeper insertion. Diseases affecting the flesh, blood aspect, bones, or organs all require deep insertions.
Needle insertion practice: The best way to practice the insertion techniques described above is to start with by needling a tightly bound pad of paper, a ball of cotton cloth, or a tightly bound piece of sponge rubber. Beginning with a 1-inch 30-gauge needle, students can gradually progress to longer and thinner needles. After they can easily insert thin needles into the practice material, they may then begin to practice on their own legs and arms. Points such as LI-11 (qū chí), TB-5 (wài guān), ST-36 (zú sān lǐ), and GB-34 (yáng líng quán) are good points for practice. The next step is to practice needle insertion on fellow students. Again, points on the limbs are the safest ones to begin with, followed by points on the body and head. This practice should be supervised by a qualified teacher.
Needle removal (出针法 chū zhēn fǎ)
The speed of withdrawal and other particulars of needle withdrawal are dependent on whether one wishes to supplement or drain the point in question. The following guidelines hold true regardless of the type of effect desired in treatment of the point.
- The needle should be rotated slightly as it is withdrawn to prevent its adhesion to body tissues.
- The needle should be withdrawn to just below the skin and then retained at this depth for a few seconds before it is fully withdrawn. This procedure will generally prevent bleeding and reduce post-needling pain.
- An alcohol-soaked ball of cotton should be used to swab the point after the needle is withdrawn.
- Needles inserted in the region of the eye should be withdrawn slowly and with special care.
Needle Manipulation Techniques
These fall into two categories: those used to facilitate the obtaining of qì and those used to control the therapeutic effect, notably supplementation and drainage.
Obtaining Qì
Obtaining qì
(得气 dé qì) and moving qì (行气 xíng qì):Obtaining qì refers to the sensation produced when a point is needled. The sensation can be described as soreness, aching, distension, heaviness, numbness or tingling depending on the point in question and the condition of the patient. This should not be confused with the superficial sensation of pricking pain that may accompany needle insertion. Obtaining qì, sometimes also called arrival of qì,
is a deeper sensation that is duller in nature and less localized than the sharp pain associated with the stimulation of subcutaneous nerves.
It is best for the practitioner to rely on the subtle physiological manifestation of qì sensation rather than on patient reports, since some patients report the slightest sensation to avoid further probing by the acupuncturist. The Biāo Yōu Fù (标幽赋 Prose Poem to Elucidate Mysteries
) states that when qì arrives the practitioner can feel a sudden deep tightness that resembles the feeling of a fish biting on a fishing line. It also states that where the needle moves easily, qì will not arrive.
Because effective treatment in Chinese acupuncture is dependent on obtaining qì, the following supplemental needling methods have been devised to aid the practitioner.
Channel-freeing manipulation (循摄法 xún shè fǎ): When a satisfactory sensation cannot be produced at the point, the practitioner presses lightly above and below the point along the course of the channel to hasten the movement of qì and blood in the channel and the subsequent arrival of qì.
Needle flicking (弹针 tán zhēn): If qì does not arrive the practitioner may lightly flick the handle of the needle, thus causing its body to vibrate and hasten the arrival of qì. Should the practitioner fail to obtain qì at a given point, it may be because of incorrect location. It is advisable to withdraw the needle and carefully relocate the point. If the channel qì is insufficient and qì fails to arrive, then the twirling and/or thrusting and lifting methods mentioned previously may be performed several times with the goal of moving the channel qì and blood and promoting the arrival of qì. If this is unsuccessful, then the channel-freeing and flicking methods will generally be successful in stimulating the arrival of qì. Should all these methods fail, it is necessary to determine if the lack of response is due to constitutional vacuity or blockage in the channels. In the former case, it is necessary to supplement the body through stimulation of points where qì can be obtained. For patients undergoing longer-term treatment, acumoxatherapy can be complemented with medicinal therapy to supplement source qì. If the channel suffers blockage, other points on the affected channel may be needled with the aim of freeing the channel and moving qì and blood.
if the disease is distant (from the point), it is necessary first to move qì to the site of disease.
This method can be employed with distant points to cause the arrival of qì sensation to travel along the channel to the affected area. To achieve this effect, the needle is inserted at a 45° angle pointing toward the disease site, and after qì is obtained the acupuncturist presses firmly on the side of the point opposite to the disease site with the thumb of the pressing hand. This moves qì in the proper direction.
Manipulation to control therapeutic effect
After the proper depth of insertion has been reached, the point can be stimulated. Stimulation methods vary according to schools of practice, but most methods are variations of the following three:
Lifting and thrusting (提插法 tí chā fǎ): After qì has been obtained, the needle is lifted a short distance (dependent on the depth of the flesh at the point) and then thrust back to the original depth. The direction of insertion should remain constant to avoid localized pain or post-needling pain. The usual distance covered by this motion is 0.3–0.5 cùn. Care should be taken to avoid raising the needle too far and thus withdrawing the needle or thrusting it too deeply and surpassing the recommended needling depth.
When employing this method strong, quick movements provide a draining stimulation, and slow, light ones are supplementing in nature.
Twirling or
Rotating the needle rapidly in a wide arc is a draining stimulation, a lesser arc and slower motion provides a supplementing stimulus.
The rotation method can be combined with the lifting and thrusting method described above.
Needle retention (留針 liú zhēn): In modem practice needles are often left in place for a period of time ranging from several minutes to two hours depending on the particular condition, although 15–30 minutes is the norm. This allows for application of other stimulation methods such as warming the needle, electrical stimulation, or intermittent stimulation. Often the needles are retained with little or no additional manipulation.
Needle retention in general can increase the ability of a point to relieve pain and quiet the spirit. Some specific treatments require needle retention to achieve satisfactory results. For example, treatment of appendicitis or asthma generally involves the retention of needles for at least half an hour.
While the needles are in place the patient must be reminded not to move. Should he move slightly, the resulting pain can be relieved by withdrawing the needle to the level just beneath the skin, and then reinserting it to its proper depth.
Classical methods for supplementation and drainage: The ancient Chinese texts list many factors that contribute to the supplementing or draining of a point. Many modern practitioners feel that this is mostly superstition and pay attention only to the strength of the stimulus, employing strong stimuli for strong patients and repletion diseases, and mild ones for weaker patients and vacuity diseases. The more important supplementing and draining methods mentioned in the Nèi Jīng and other texts are summarized in Needle Manipulation tables below.
One classical scheme for supplementation and draining is rests on the exuberance and debilitation of qì in the channels at different watches (two-hour periods) of the day. To supplement, needle when the channel qì is debilitated (the watch immediately following exuberance). To drain, needle when the channel is exuberant. The times of exuberance of the qì of each channel are as follows.
- 0300–0500 hrs (B3寅时 yín shí): Hand greater yīn (tài yīn) LU
- 0500–0700 hrs (B4 卯时 mǎo shí): Hand yáng brightness (yáng míng) LI
- 0700–0900 hrs (B5 辰时 chén shí): Foot yáng brightness (yáng míng) ST
- 0900–1100 hrs (B6 巳时 sì shí): Foot greater yīn (tài yīn) SP
- 1100–1300 hrs (B7 午时 wǔ shí): Hand lesser yīn (shào yīn) HT
- 1300–1500 hrs (B8 未时 wèi shí): Foot greater yáng (tài yáng) SI
- 1500–1700 hrs (B9 申时 shēn shí): Foot greater yáng (tài yáng) BL
- 1700–1900 hrs (B10 酉时 yǒu shí): Foot lesser yīn (shào yīn) KI
- 1900–2100 hrs (B11 戌时 xū shí): Hand reverting PC
- 2100–2300 hrs (B12 亥时 hài shí): Hand Lesser yáng (shào yáng) TB
- 2300–0100 hrs (B1 子时 zǐ shí): Foot lesser yáng (shào yáng) GB
- 0100–0300 hrs (B2 丑时 chǒu shí): Foot reverting yīn (jué yīn) LR
The above methods of supplementation and drainage are not a subject of unanimous agreement. Through the ages different opinions have been proffered. They are presented here as an introduction to the subject, realizing that each practitioner must develop his or her own preferences in these matters.
In addition, supplementation and draining can be achieved using mother and child points on the basis of five-phase theory.
Combined methods of supplementation and drainage:While there are many methods that combine the above-mentioned techniques, the present discussion covers only the two that are most commonly employed. These methods, one supplementing and one draining, involve manipulating the needle between three depths known as heaven, earth, and human. Heaven is the level just below the skin; earth is the level of deepest insertion; and human is the intermediate level.
Burning mountain fire method (烧山火法 shāo shān huǒ fǎ): To perform this technique, insert the needle into the heaven level and then thrust and lift nine times, thrusting forcefully and lifting gently. Then proceed to the human level and repeat this procedure. Finally, enter the earth level and once again repeat the lifting (gently) and thrusting (with force) motion nine times. When this has been done, lift the needle in one slow motion to the heaven level. If a warm, slightly burning sensation has not been achieved, the entire procedure may be repeated three times. If, at that time, the sensation still does not arrive, the practitioner should cease manipulation for a moment and then repeat the above procedure until the appropriate sensation occurs. When removing the needle, the needling site should be covered.
This is a supplementing method that combines the supplementing aspects of the quick and slow, lifting and thrusting, six-nine, and open and closed and covering methods outlined in the two Needle Manipulation tables below. Further supplementation can be achieved by inserting the needle while the patient exhales and withdrawing it during inhalation. The burning mountain fire method is named for the burning sensation it produces and is useful for supplementing qì of the channels and organs. It can be employed to treat vacuity cold diseases such as the three yīn stages of cold damage disease, impotence, incontinence, yīn protrusion (prolapse of the uterus), and swelling and sagging of one testicle.
Step 1: Determine the depth to which the needle will be inserted. Divide this depth into three equal segments. From the surface of the skin, these depths are called the heaven level, the human level, and the earth level.
Step 2: Ask the patient to inhale deeply. Steps 2, 3, and 4 are performed during exhalation. Upon exhalation, thrust the needle quickly and lift slowly nine times to the heaven level.
Step 3: Thrust the needle quickly and lift slowly nine times in the human level.
Step 4: Thrust the needle quickly and lift slowly nine times in the earth level.
Step 5: Ask the patient to inhale, and slowly withdraw the needle. If the procedure is to be repeated, withdraw the needle to the heaven level and repeat steps 2, 3, and 4; if not, withdraw the needle fully from the skin.
Step 6: Press the acupuncture site gently with a ball of cotton wool after the needle has been withdrawn.
This is a draining method that combines the draining aspects of the lifting and thrusting, slow and quick, 6 and 9, and opening and covering methods. Further draining can be achieved by inserting the needle on inhalation and withdrawing it as the patient exhales. The penetrating heaven cooling method courses and drains yáng exuberance and evil qì. It is employed to treat repletion febrile disease, wind block, warm malarial disease, mania and withdrawal, summerheat strike, and high fever.
Step 1: Determine the depth to which the needle will be inserted, and divide this depth into heaven, human, and earth levels as described above.
Step 2: Ask the patient to inhale deeply and slowly. (Steps 2 through 6 are performed during inhalation.) Insert the needle to the earth level.
Step 3: Thrust slowly and lift quickly in the earth level six times.
Step 4: Bring the needle up to the human level. Thrust slowly and lift quickly in the human level six times.
Step 5: Bring the needle up to the heaven level. Thrust the needle slowly and lift the needle quickly in this level six times.
Step 6: Repeat steps 3 through 5.
Step 7: Ask the patient to exhale, and withdraw the needle quickly, leaving the point uncovered.
Both the penetrating heaven cooling method and the burning mountain fire method are suitable only for points located in thick muscle and are not used on the head or chest. Only one or two points are commonly chosen for each method in a single treatment.
| Needle Manipulation | ||||
|---|---|---|---|---|
| Method | Description | Supplementing | Draining | Application |
| Needle Retention (留针 liú zhēn) | Leaving the needle inserted for a given period of time | Short duration | Longer duration | The two methods are often combined with one or more of the other methods. |
| Nine-Six Supplementation and Drainage (九六补泻 jiǔ liù bǔ xiè | Twirling or thrusting the needle either six or nine times | Intervals of nine twirls/thrusts | Intervals of six twirls/thrusts | |
| Directional Supplementation and Drainage (迎随补泻 yíng suí bǔ xiè) | Angling the needle with or against the flow of qì | Angling the needle in the direction of qì flow | Angling the needle against the qì flow | These two methods are suitable for harmonizing provisioning and defense, coursing and freeing the channels, and relieving pain, itching, and numbness. |
| Twirling Supplementation and Drainage (捻转补泻 niǎn zhuàn bǔ xiè) | Rotating the needle with or against the flow of qì | Hand three yáng and foot three yīn clockwise | Hand three yáng and foot three yīn counterclockwise | |
| Hand three yīn and foot three yáng counterclockwise | Hand three yīn and foot three yáng clockwise | |||
| Slow and Quick Supplementation and Drainage (徐疾补泻 xú jí bǔ xiè) | Speed of insertion and of withdrawal | Slow, deliberate insertion and rapid withdrawal (withdraw quickly to just below the surface of the skin, then withdraw completely) | Rapid insertion and slow withdrawal | These four methods are use to harmonize yīn and yáng, eliminate superabundance and insufficiency, and treat heat or cold conditions. |
| Lifting and Thrusting Supplementation and Drainage (提插补泻 tí chā bǔ xiè) | Strength of the lifting and thrusting motion after insertion | Thrust forcefully and lift gently | Thrust gently and lift slowly | |
| Respiratory Supplementation and Drainage (呼吸补泻 hū xī bǔ xiè) | Insertion or withdrawal in accordance with the breath | Insert during exhalation and withdraw during inhalation | Insert during inhalation and withdraw during exhalation | |
| Open and Closed Supplementation and Drainage (开阖补泻 kāi hé bǔ xiè) | Encouraging or preventing the escape of qì after needle removal | Preventing the escape of qì by pressing on the insertion puncture after needle removal | Encouraging the escape of qì by waggling the needle to leave a wider hole after needle removal | |
Precautions, Contraindications, and Mishaps
Needling precautions
Regarding specific precautions, it should be remembered that acupuncture has some inherent dangers that can only be mitigated by the constant attention of the practitioner. Most important are the cautions listed below.
- The practitioner should be familiar with the locations of the internal organs and the appropriate needling depths associated with points in those areas. This precaution includes the sense organs and sex organs.
- The practitioner must be familiar with the location of major blood vessels in the area of points to avoid puncturing them.
- When treating pregnant women, the needling of points in the abdomen, lower back, and sacral region is prohibited. In addition, needling SP-6, LI-4, ST-12, GB-21, BL-67, and BL-60 is contraindicated after the first trimester of pregnancy.
- The Nèi Jīng warns against performing acupuncture in the hours before or after the patient has had sexual intercourse, eaten, drunk alcohol, or traveled a long distance, or if the patient is in a state of great fright or anger.
- Several points are forbidden to needle or moxa. The practitioner should be familiar with these restrictions and the reasons these points have contraindications. Physicians of the past had little understanding of anatomy, and the needles they used were cruder than those employed in modern practice. They thus forbade needling of many points that can in reality be needled superficially without danger. The list below includes the points stipulated as forbidden to needle in most older texts. The points with double asterisks (⁑) are still classed as prohibited in modern practice.
Points Contraindicated for Needling
- GV-24: This point is now commonly needled 0.2–0.3 cùn.
- GV-17: Modern sources needle to 0.3 cùn.
- BL-9: Currently needled 0.3 cùn.
- BL-8: Currently needled 0.3–0.5 cùn.
- GB-18: Currently needled 0.3–0.5 cùn.
- TB-19: Currently needled 0.1 cùn.
- TB-20: Currently needled 0.1 cùn.
- ST-1: Currently needled 0.2–0.3 cùn; it can create a black eye.
- GV-11: Some modern sources say a 0.5–1. 0 cùn insertion is acceptable.
- GV-10: See GV-11.
- CV-17: Now needled to a depth of 0.3–0.5 cùn.
- LI-13⁑: Site of the radial collateral artery and vein.
- HT-2: Currently needled 0.3–0.5 cùn.
- CV-8⁑: This is the navel. The Nèi Jīng mentions that needling this point will cause the patient to have a festering navel ulcer, most likely because the navel is susceptible to infection.
KI-ll : Currently needled 0.5–0.8 cùn.- ST-30: This is the site of a major artery; currently needled 0.3–0.5 cùn.
- SP-11: Currently needled 0.3–0.5cùn; it is the site of a major vein and artery.
- BL-56: Some modern sources needle this point 1. 0–1.5 cùn.
- CV-9: Currently needled 0.5–1. 0 cùn. Should not be needled to treat water swelling (employ moxibustion instead).
- CV-1: Currently needled 0.5–0.8 cùn.
- ST-17⁑: This is the nipple.
- TB-8: Some modern sources needle this point 0.5–1. 0 cùn.
- LR-12⁑: Site lies on the femoral artery.
Needling Mishaps
Untoward responses to needling are uncommon when proper protocols are followed. They include needle sickness, stuck needle, bent needle, broken needle, and hematoma.
Needle sickness (晕针 yùn zhēn): The signs of needle sickness are somber-white complexion, dizziness, panic, shortness of breath, oppression in the chest, and a fine sunken pulse. In serious cases, there may be reversal cold of the limbs, loss of consciousness, urinary and fecal incontinence, and a faint pulse on the verge of expiration. Needle sickness may result from constitutional weakness, nervousness, fatigue, hunger, severe sweating, severe diarrhea, or major blood loss. It is prevented by making sure the patient is relaxed, is not hungry (but not full), and by using light needle stimulus, especially with first-time patients. It is managed by ceasing needling or removing the needles, by allowing the patient to lie flat or lower the head, and by loosening their clothing. This is usually sufficient for the patient to recover. In severe cases, GV-26 (shuǐ gōu), PC-6 (nèi guān), KI-1 (yǒng quán), and ST-36 (zú sān lǐ) can be needled and GV-20 (bǎi huì), CV-6 (qì hǎi), and CV-4 (guān yuán) can be moxaed to revive the patient.
Stuck needle (滞针 zhì zhēn): A needle is described as stuck
when there is difficulty in twirling, lifting and thrusting, or removing the needle. If these actions are forced, then patient may experience pain.
Stuck needle has several causes: excessively vigorous needle manipulation; uneven twirling or lifting and thrusting; continual twirling in one direction; muscle fibers catching the needle; muscular spasm due to nervousness or other factors; or incorrect angling of the needle.
If stuck needle occurs as a result of the patient’s nervousness, it can be managed by stopping any manipulation, by rubbing the area surrounding the needling site, or by flicking the needle, or inserting another needle close to the one that is stuck. If due to continual twirling in one direction, the practitioner should turn the needle in the opposite direction and try scraping or flicking the needle.
Stuck needle is prevented by ensuring that patient remains relaxed and by proficiency in needle manipulation.
Bent needle (弯针 wān zhēn): A needle may bend as a result of poor needling skills, excessively vigorous manipulation, or forcing the needle into firm tissues. Bent needle may also occur if the patient changes his posture after needle insertion, or if the needle is accidentally pressed or knocked. It may also result from failure to cope with stuck needle.
If the needle is slightly bent, it can usually be gently withdrawn and removed. If severely bent, it can be waggled gently and withdrawn following the direction of the bend. If a bent needle is caused by a change in the patient’s posture, the original posture should be restored and the surrounding muscles should be allowed to relax so that the needle can be gradually withdrawn and removed. Any forced removal of the needle can result in breakage.
Bent needle can be avoided by proficiency in needle manipulation, by preventing any pressure or impacts on the needle, and by ensuring that the patient does not change posture.
Broken needle (折针 zhé zhēn): This is when the needle breaks either above the skin and within the flesh. This happens owing to the following factors: poor quality needles; forced twirling or lifting and thrusting giving rise to vigorous contraction of muscles; insertion of the needle up to the handle; changes in the patient’s posture; impact by an external force; failure to manage stuck needle or bent needle; or sudden bursts of power in electroacupuncture.
If a needle breaks during treatment, the patient should be told to maintain the original posture and not move in order to prevent the needle from moving deeper into the flesh. If the breakage is above the skin, the needle can be removed with tweezers. If the break point is level with the skin surface or just below it, the surrounding skin can be pressed using the thumb and index finger of one hand so that the needle is pushed out far enough to be removed with tweezers using the other hand. A breakage deep below the skin can only be removed surgically.
Broken needle can be prevented by inspection of the quality of needles before insertion, by proficiency in needle manipulation, and proper management of the patient’s posture, and prevention of impact accidents (objects accidentally dropping on the needle).
Hematoma (血肿 xuè zhǒng): A hematoma occurs when a needle punctures a blood vessel, causing extravasation that gives rise to green-blue or purple macules below the surface of the skin. This often happens when the tip of the needle is bent.
In mild cases, the hematoma will clear in time without treatment. More severe cases can be treated by applying a cold compress followed by a hot compress or by gentle rubbing of the affected area. Hematomas can be avoided by needle quality inspection and by proficiency in needling.
Other Materials and Techniques Related to Acupuncture
Bloodletting (放血 fàng xuè) with a three-edged needle (三稜針 sān léng zhēn): The three-edged needle (sometimes called the prismatic
or ensiform needle
) is a thick needle with a sharp, three-edged tip used for letting blood. The use of pre-sterilized, disposable lancets has replaced the three-edged needle for bloodletting in many acupuncture clinics. Bloodletting employs the three-edged needle to puncture the skin and allow the escape of a few drops of blood. It is performed at the site of a point or at the small veins in the area surrounding a point (such as BL-40). The function of this method is to drain heat or quicken the blood and qì and relieve local congestion (and thus reduce stagnation and swelling).
This procedure is done by first applying pressure to restrict the blood flow of the area, to increase the visibility of the veins, and to cause the blood to flow out more easily when the vein is pricked. The point is then swiftly and decisively pricked to a superficial depth of about 0.1 cùn and a few drops of blood are allowed to escape. Lastly, the point is pressed with sterile cotton until the bleeding ceases.
This method is inappropriate for weak, pregnant, or postpartum patients, hemorrhagic patients, and patients suffering from anemia or low blood pressure. The procedure should be thoroughly explained to the patient before it is performed to allay his or her fears. Furthermore, strict attention must be paid to sterile technique and careful cleaning of the puncture site before and after pricking.
The following list indicates some diseases that respond to bloodletting. Double asterisks mark indications for which this procedure is most commonly employed. The suggested points should be combined with standard acupuncture and moxibustion therapy to obtain the best results.
- Wind stroke⁑: BL-40, LI-4, GB-21
- Cholera: BL-40, LU-5, LI-11
- Spasm of the gastrocnemius: SP-1
- Cough (with phlegm): LI-11, LU-5
- Headache: ST-8, GV-20
- Stomach (Stomach duct) pain: BL-38
- Abdominal pain: LR-1
- Food damage: GV-20
- Jaundice: SP-1, BL-20, BL-21
- Spinal pain: BL-38
- Rib-side pain: BL-18
- Mounting qì (shàn qì,hernia): BL-23
- Mouth and tongue ulcers: HT-7
- Swelling of mouth, tongue, or pharynx: LI-11
- Toothache: LI-4
- Wind, swelling and pain⁑ (in eyes): ST-8
- All eye diseases: BL-18, ST-8, LU-11, GV-20
- Sore throat⁑: LU-11
- Drinker’s nose⁑: LU-7, LI-4
- Strangury diseases: SP-6, BL-40
- Leg qì: BL-57
- Shoulder pain: BL-13
- Itching over the entire body: LI-4, GV-20
- Breast swelling and pain (in women): BL-38
- Menstrual clots: BL-40
- Child gān disease: BL-18, BL-17, BL-21, GV-12, M-BW-24 and
M-UE-9 - Cinnabar toxin (dān dú): BL-40, BL-17
The cutaneous needle (皮内针 pí nèi zhēn): The seven-star or plum-blossom needlecan be used to tap the skin of the affected area or along channel to treat disorders associated with the channel. This method is of particular value for treating children and others where pain or fear of needle insertion may be a factor. The tapping can be of a light (no bleeding) or heavy (slight bleeding) nature depending on the patient’s condition and the type of disease being treated. In modern China heavy tapping is employed to move stagnant blood in a local area. Legal and cultural factors limit the applicability of this method in the West. This is compounded by the inability of some cutaneous needles with plastic handles to undergo sterilization. Nonetheless, use of light cutaneous tapping for treatment of children and adults is certainly of clinical value. Digestive disorders, headache, menstrual pain, and some skin diseases respond well to this type of treatment.
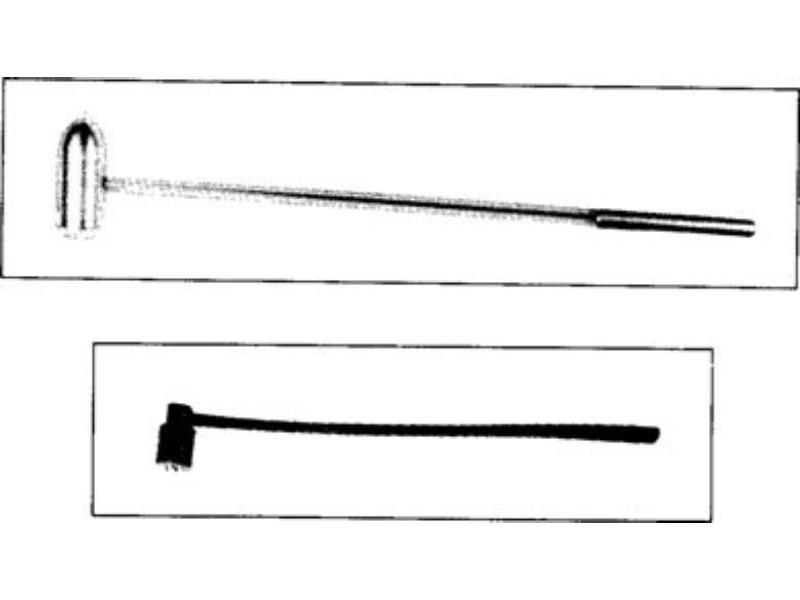 |
| Seven star needle |
|---|
The needle should be held about two cùn above the skin and manipulated by a loose movement of the wrist. The needle must strike the skin perpendicularly and without excessive force in order to prevent bleeding. In general, tapping is performed from the top downward and from the medial toward the lateral aspect. Cutaneous tapping is contraindicated over ulcerations or traumatic injuries.
Intradermal needle (皮内针 pí nèi zhēn): Intradermal needles are available in two types. The wheat-grain type is straight with a small grain-shaped handle. It is inserted transversely into the skin to a depth of about 1 cm. and the handle is then held flat against the skin by adhesive tape. These needles are generally inserted in the back or limbs and treat various types of chronic, stubborn, or painful disorders such as migraine headache, back pain, stomach pain, asthma, and menstrual irregularities.
The
Implantation of intradermal needles is aided by the use of tweezers because these needles are very small. The needles are retained generally from 1 to 3 days—shorter periods in warm weather, and longer periods in cold weather. The patient should be encouraged to keep the area of insertion clean to avoid infection.
Electroacupuncture (电针 diàn zhēn): Electroacupuncture involves attaching wires between two needles and applying an electrical current to them. It is most commonly used for treating pain. In China, it is sometimes used to provide anesthesia during surgery.
Selecting and Combining Needling Points
See the following:
Back to search result Previous Next